We are open to partnering, contact our team at
Phase 2-ready oral p38 MAP kinase inhibitor
Influenza affects around a billion people each year. Compared to other respiratory viral infections, the symptoms of influenza can be more severe and it is commonly detected in patients hospitalised for severe acute respiratory infections 1, 2,3.
Severe influenza is typically characterised by a disproportionate systemic immune response, which can cause significant local damage in the lungs and can affect other organs in the body. The uncontrolled immune response commonly results in a need for hospitalisation and carries a mortality risk.
Although triggered by the viral infection, the aggressive hypercytokinaema can exacerbate pathological damage and lead to life-threatening multiple organ dysfunction syndromes 4. In most cases, death is caused by the body trying to heal itself 5. Existing influenza treatments disrupt viral life cycle but do not remedy rampaging immune response which drives severe disease. POLB 001 is a paradigm shift in the treatment of severe influenza by bringing the immune system back into check and allowing it to effectively clear the virus while reducing its deleterious effects on the body.
Compelling Data
- Phase 2-ready oral small molecule, excellent bioavailability
- Strong pre-clinical data package
- Proven safety profile & well tolerated in Phase 1 clinical trial
- Efficacy demonstrated in Phase 1b human challenge trial supports partnering
Strong Patent Portfolio
- Granted patents for severe influenza with a term of protection to at least 2038
- Dosage regime patent application filed in 2023, potential for protection to at least 2044
- Oncology patent applications filed in 2023, potential for protection to 2044
- Learn more about POLB 001 for cancer immunotherapy-induced CRS here
Major Market Opportunity
- 1 billion estimated cases of influenza each year, with 3-5 million severe cases, causing 290,000 to 650,000 respiratory deaths annually5
- Current treatments are effective within the first 48 hours of symptom onset but are less effective at more advanced stages of the disease6
- POLB 001 is influenza strain agnostic and shelf stable making it ideal for potential stockpiling
Evidence for benefit of POLB 001 in the therapy of LPS-induced inflammation
Supplementing the applicability of POLB 001 to severe influenza on the one hand and immunotherapy-induced CRS on the other, POLB 001 has been investigated in a human lipopolysaccharide (LPS) challenge trial to review its clinical activity to prevent or dampen harmful immune responses.
Randomised, double-blind, placebo-controlled, multiple dose, inflammatory challenge trial in healthy volunteers
Trial design

Endpoints
Intravenous LPS challenge
- Bloods (cytokines, vascular markers, CRP)
- Ex-vivo LPS response
- Safety & tolerability (inc. vital signs, AE’s, ECG, Haematology)
Local inflammatory responses were also measured following intradermal LPS challenge
LPS Challenge Trial Results Demonstrate POLB 001 can Potently Inhibit Inflammation
POLB 001 was widely distributed, reduced the inflammatory response and inhibited p38 MAPK activation and signaling following LPS challenge.
- Excellent safety profile across two clinical trials
- Potent target inhibition confirmed
- Major reduction of key inflammatory markers
- Clear dose response relationship observed
Potent and Selective Inhibition of p38 MAPK Signaling
Potent and Selective Inhibition of p38 MAPK Signaling
Effective target engagement demonstrated in LPS human challenge trial

Levels of phosphorylated p38 MAPK in circulating monocytes
- POLB 001 was widely distributed
- POLB 001 inhibited p38 MAPK activation, direct measurement of activation
- POLB 001 inhibited in vivo and ex vivo responses to LPS-induced TNF-α, indirect measurement p38 activity
Blood samples were taken before and after administration of intravenous LPS. Peripheral blood samples were analysed by flow cytometry. Monocytes were gated by FSC, SSC and CD14+. Data is presented as mean MFI values of phospho-p38 +/- SEM
Reduced Key Inflammatory Cytokines Following LPS Challenge
Reduced Key Inflammatory Cytokines Following LPS Challenge
Dose dependent reductions, without ablation of immune system, leaving key immune functions intact
TNF-α

TNF-α reduction of 73.5% and 56.2% seen for 70 mg and 150 mg doses respectively (p = 0.0003†)
IL-6

IL-6 reduction of 57.4% and 63.5% seen for 70 mg and 150 mg doses respectively (p = 0.0002†)
IL-8

IL-8 reduction of 80.7% and 76.7% seen for 70 mg and 150 mg doses respectively (p < 0.0001†)

TNF-α, IL-6 and IL-8 levels decreased between 56-81% in subjects treated with 70 mg or 150 mg POLB 001 twice daily
†The exploratory analysis suggested statistically significant improvement in treatment (p<0.05) for the endpoints examined.
Reduced Key Indicators of LPS-Induced Systemic Inflammation
Reduced Key Indicators of LPS-Induced Systemic Inflammation
The reduction of systemic cytokines align with improvement in clinically meaningful endpoints
Mean Body Temperature

No significant effect on body temperature with a trend towards reduction compared to placebo.
Heart Rate Rise (bpm)

Suppressed increase in heart rate following IV LPS administration
C-Reactive Protein (CRP)

CRP level reductionof 33.1% and 33.3% seen for 70mg and 150mg doses respectively
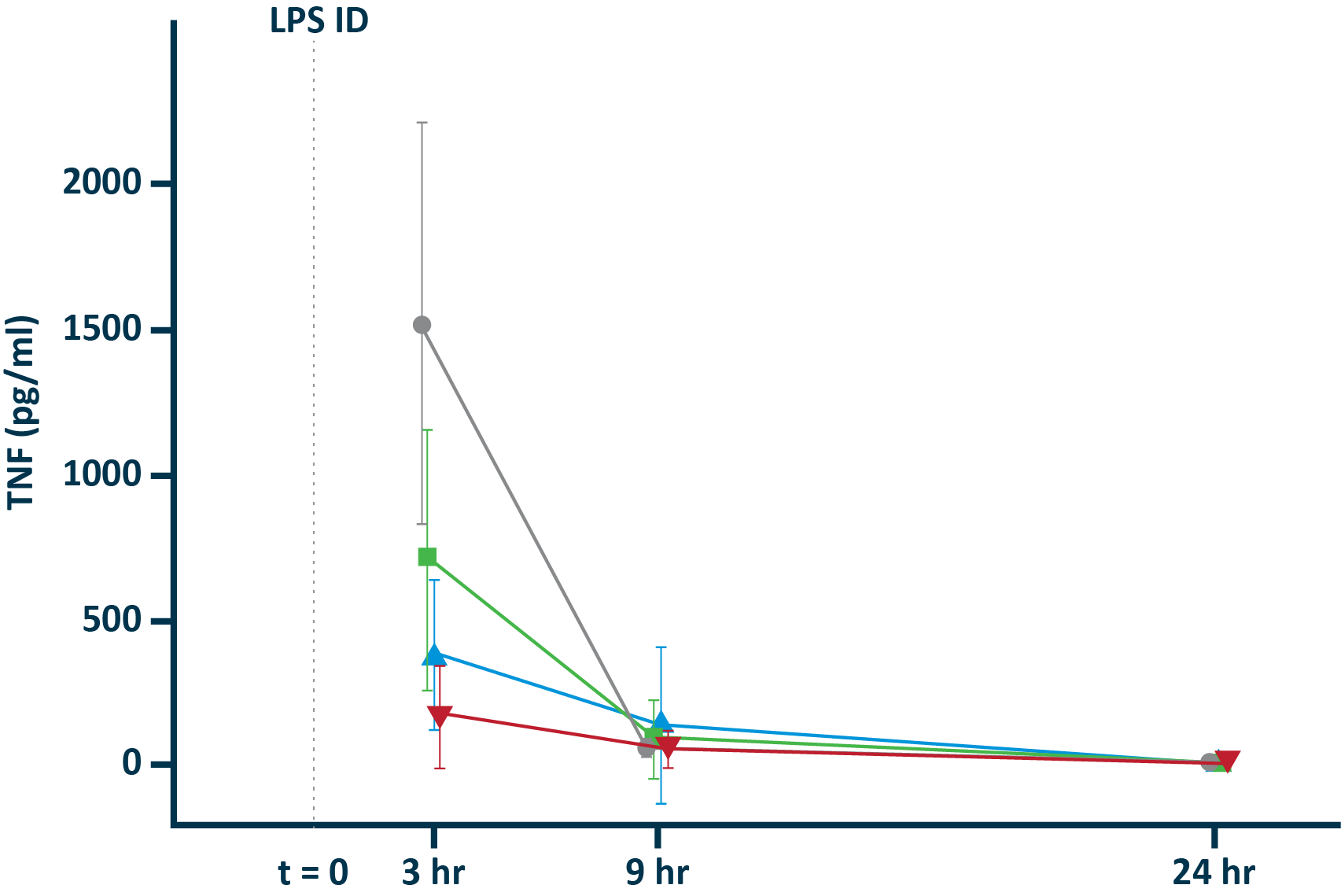
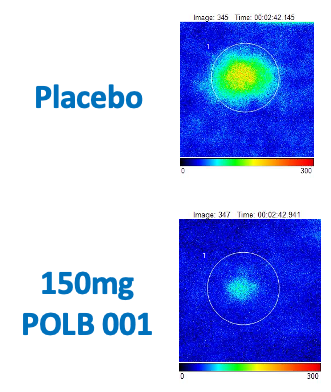
POLB 001 Effectively Reduced Inflammation in Tissue
POLB 001 Effectively Reduced Inflammation in Tissue
POLB 001 significantly reduced IL-1β† and TNF-α† responses in blister exudate compared to placebo
TNF-α in blister exudate
IL-1β in blister exudate
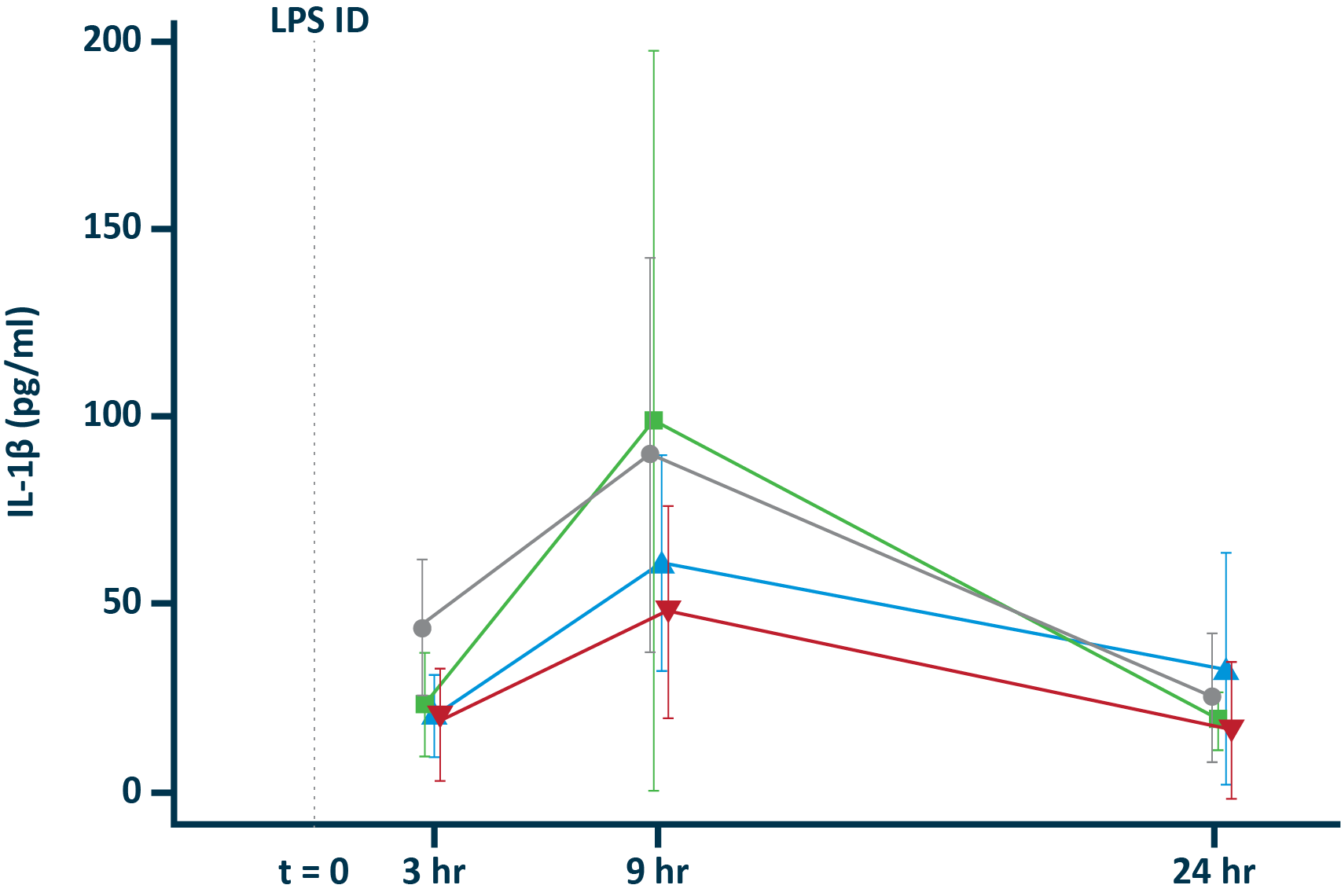
†The exploratory analysis suggested statistically significant improvement in treatment (p<0.05) for the endpoints examined.
References
- https://www.nature.com/articles/s41598-021-84423-2. This paper looks at the differences in clinical severity of various respiratory viral infections. It attributes a clinical severity score (CSS) and Flu A was the most severe. “CSS ranged from a mean of 1.83 (IQR 1, 2) for HRV to 2.74 (IQR 2, 3) for Flu A”.
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7018304/. See title and table 3. Together they support influenza being responsible for the highest number of severe acute respiratory infections in adults.
- https://www.nature.com/articles/s41598-024-55378-x See methods to see that all patient records were included in a certain time period (i.e. no selective recruitment) and see table 1 for a break down of causes. Of 807 patients, 332 had covid and 324 had influenza. This supports statement that it is one of the most common causes of ICU hospitalisation.
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8310017/
- https://www.scientificamerican.com/article/how-does-the-flu-actually-kill-people/ See “But what exactly is a “flu-related death”? How does the flu kill? The short and morbid answer is that in most cases the body kills itself by trying to heal itself. “Dying from the flu is not like dying from a bullet or a black widow spider bite,” says Amesh Adalja, an infectious disease physician at the Johns Hopkins University Center for Health Security”
- World Health Organization, October 2023.
- National Foundation of Infectious Diseases, September 2024.